Piperacillin,Tazobactam
Overview
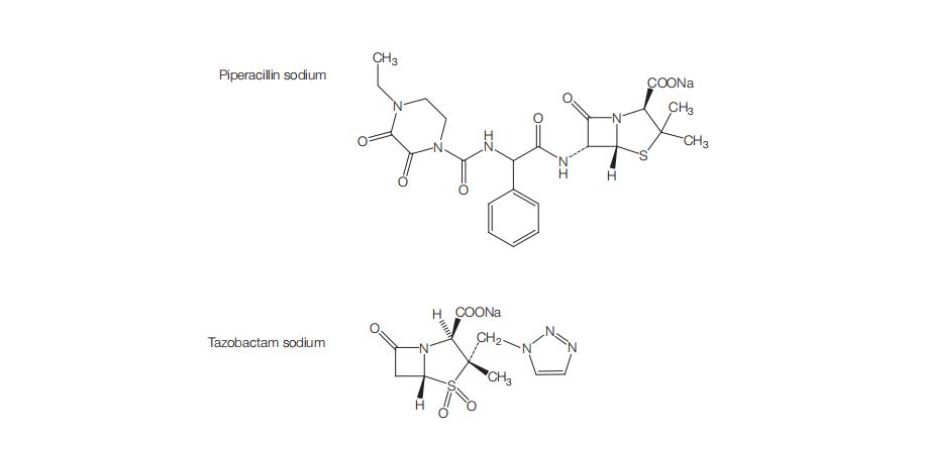
Piperacillin‑tazobactam is a combination antibacterial medication consisting of the extended‑spectrum ureidopenicillin antibiotic piperacillin and the β‑lactamase inhibitor tazobactam administered by intravenous infusion. Piperacillin exerts bactericidal activity by inhibiting bacterial cell wall synthesis, and tazobactam enhances this effect by inhibiting many β‑lactamases that would otherwise inactivate piperacillin. This combination expands the spectrum of activity to cover a wide range of Gram‑positive, Gram‑negative, and anaerobic bacteria, including many β‑lactamase producing strains that contribute to complicated infections in hospitalized patients. The medication is typically used in settings of moderate to severe infections such as intra‑abdominal infections, skin and skin structure infections, nosocomial and community‑acquired pneumonia, and gynecologic infections, with dosing and duration guided by severity and pathogen susceptibility. The intravenous route and dosing frequency are selected to maintain serum concentrations above the minimum inhibitory concentrations for susceptible organisms, and careful clinical monitoring supports effective therapy while minimizing toxicity. Piperacillin‑tazobactam remains a cornerstone in empiric and directed therapy for serious infections in both adults and pediatric patients.
Background and Date of Approval
Piperacillin‑tazobactam was first approved for medical use in the United States by the Food and Drug Administration in 1993, marking its introduction as a combination antibacterial agent for serious bacterial infections requiring broad‑spectrum coverage. Since initial approval, it has become widely adopted in clinical practice and included on essential medicines lists due to its utility against challenging hospital‑associated pathogens. Regulatory approvals in multiple regions, including the United States and other international authorities, reflect its established role in treating infections where β‑lactamase production by bacteria compromises the efficacy of standard penicillins. Over the decades, adjustments in susceptibility breakpoints and dosing recommendations have been informed by evolving microbiologic data and clinical experience to optimize its clinical use against a broad range of pathogens. Piperacillin‑tazobactam’s continued availability and guideline inclusion underscore its relevance in current antimicrobial therapy.
Uses
Piperacillin‑tazobactam is indicated for treatment of a variety of bacterial infections in adults and pediatric patients aged two months and older. These include complicated intra‑abdominal infections such as appendicitis with rupture or abscess and peritonitis, complicated and uncomplicated skin and skin structure infections including diabetic foot infections, moderate community‑acquired pneumonia, nosocomial pneumonia including hospital‑associated infections, and female pelvic infections such as postpartum endometritis and pelvic inflammatory disease. The combination is used when infections are caused by β‑lactamase producing organisms or when broad‑spectrum empirical coverage is warranted, and it may be used in conjunction with other agents such as aminoglycosides in selected severe infections to extend coverage.
Administration
Piperacillin‑tazobactam is administered by intravenous infusion, with typical adult dosing for most indications comprising 3.375 grams (equivalent to 3 grams of piperacillin and 0.375 grams of tazobactam) every six hours infused over approximately 30 minutes, or 4.5 grams every six hours for more severe infections such as nosocomial pneumonia, often in combination with an aminoglycoside when Pseudomonas aeruginosa is a concern. Treatment durations generally range from seven to ten days for many infections and up to 14 days for complicated nosocomial pneumonia, with adjustments based on clinical response and culture results. Renal impairment necessitates dose adjustments, and pediatric dosing for patients aged two months and older follows weight‑based recommendations, with careful monitoring of renal function and infusion tolerability throughout therapy.
Side Effects
Commonly observed adverse effects associated with piperacillin‑tazobactam include gastrointestinal symptoms such as diarrhea, nausea, vomiting, and dyspepsia, as well as local reactions at the infusion site including pain and irritation. Patients may also experience fever or transient laboratory abnormalities such as increases in liver enzymes or changes in blood counts. These side effects are generally manageable under medical supervision, and clinicians monitor patients regularly to assess for persistence or worsening of symptoms that may warrant intervention.
Warnings
Serious adverse events with piperacillin‑tazobactam can include hypersensitivity reactions, including anaphylaxis in individuals with penicillin or β‑lactam allergies, and severe cutaneous reactions such as Stevens‑Johnson syndrome or toxic epidermal necrolysis, which require immediate discontinuation. Hemophagocytic lymphohistiocytosis and rhabdomyolysis have been reported rarely. Hematologic abnormalities such as leukopenia, neutropenia, thrombocytopenia, and bleeding manifestations may occur, particularly with prolonged use. Clostridioides difficile associated diarrhea and colitis may develop during or after therapy due to alteration of normal gut flora. Piperacillin‑tazobactam should be avoided in patients with known hypersensitivity to penicillins, cephalosporins, or β‑lactamase inhibitors, and clinicians should assess allergy history carefully before initiating treatment.
Precautions
Baseline assessments prior to initiating piperacillin‑tazobactam include evaluation of renal function, allergy history, and concomitant medications. Dose adjustments are indicated in patients with impaired renal function to prevent accumulation and toxicity. Although classical pharmacokinetic drug interactions are less common with β‑lactam antibiotics, concurrent use with vancomycin has been associated with an increased incidence of acute kidney injury, and co‑administration with aminoglycosides requires separate infusion lines to avoid inactivation. Electrolyte disturbances, particularly hypokalemia, may occur and periodic monitoring of electrolytes and renal function is recommended during therapy.
Expert Tips
When selecting piperacillin‑tazobactam, clinicians should consider local susceptibility patterns and culture data to ensure appropriate empirical and targeted therapy, particularly in settings with high prevalence of resistant Gram‑negative organisms. Baseline testing should include renal function and complete blood counts, with periodic reassessment during treatment. Patient counselling should emphasize the importance of reporting rash or symptoms of allergic reactions promptly, adherence to the full course of therapy, and monitoring for signs of diarrhea that may indicate C. difficile infection. Handling considerations include ensuring appropriate storage and reconstitution per product labeling, and when used with other intravenous antibiotics, coordination of infusion times and lines reduces risks of incompatibilities and ensures optimal efficacy.